

Introduction: Mantle cell lymphoma (MCL) is a rare type of incurable B-cell lymphoma with an incidence rate of ~0.8/100,000 in the United States (US) (Blood, PMID: 30154113; CA Cancer J Clin, PMID: 27618563). Recent advances in understanding of MCL biology, development of new therapeutic modalities such as Bruton tyrosine kinsase inhibitors (BTKi), and advancement of treatment strategy incorporating chemotherapy and non-chemotherapy treatment modalities have improved survival (Am J Hematol, PMID: 30963600; Blood, PMID: 26059948; Blood, PMID: 28899853). However, prognosis for MCL remains poor overall (Blood, PMID: 30154113). Although variations in incidence in MCL by race has been reported in the literature (CA Cancer J Clin, PMID: 27618563), there is currently limited data available on differences in demographics, treatment patterns, and outcomes in Hispanic (H) MCL patients.
Methods: In this retrospective cohort study, de-identified data was obtained from the Texas Cancer Registry (TCR) database for those diagnosed with MCL between 2006-2016. Standard demographic variables collected include gender, race, ethnicity, birthplace, dates at diagnosis and death, primary payer at diagnosis, stage, type of treatment, poverty index, and vitality status among others. The significance of variation in the distribution of outcomes with ethnicity [H, non-Hispanic (NH)] was assessed with Fisher's Exact test, Pearson's Chi-square test, T-test, or Wilcoxon test as appropriate. Survival time was measured in years from date of primary diagnosis to date of death. Patients not coded as dead were considered censored on survival time at the date last seen. Survival distributions were described with Kaplan-Meier curves and significance of variation in median survival with ethnicity was assessed with log rank testing. All statistical testing was two-sided with a significance level of 0.05.
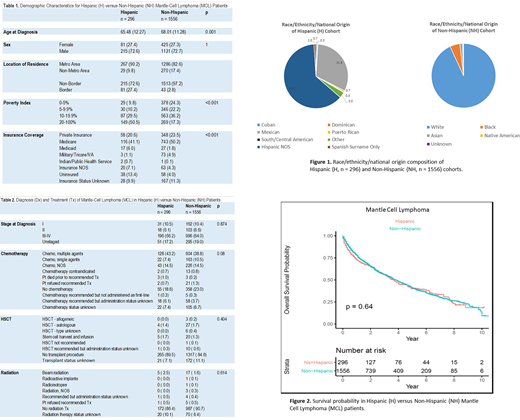
Results: A total of 1852 (296 H, 1556 NH) patients were included in the final analysis. Median age at diagnosis were 65.5 (H) and 68.0 (NH). 72.6% of H and 72.7% of NH cohorts were male. Of the NH cohort, 92.5% were White, 5.3% Black, 1.5% Asian, 0.4% Native American and 0.1% with unknown race. There was a statistically significant difference between the cohorts in the poverty index. Most H (50.5%) were in the 20-100% bracket, while the majority of NH (36.2%) were in the 10-19.9%. The majority of the cohort were from metro areas (90.2% H and 82.6% NH) and non-border counties (72.6% H and 97.2% NH). There was a statistically significant difference in insurance status at diagnosis between the cohorts. Medicare was the most common type for both H (41.1%) and NH (50.2%), while 13.4% of H and 4.0% of NH were uninsured. The majority of H (66.2%) and NH (64.0%) were diagnosed with stages 3-4 MCL; for H, stage 1 10.5%, stage 2 6.1%, stages 3-4 66.2%; for NH, stage 1 10.4%, stage 2 6.6%, stages 3-4 64.0%. The most common treatment received was combination chemotherapy (43.2% H, 38.8% NH); for H, combination chemotherapy (CC) 43.2%, single agent chemotherapy (SAC) 7.4%, chemotherapy not otherwise specified (CNOS) 14.5%, died prior to recommended treatment (PRI) 1%, refused recommended treatment (REF) 0.7%, treatment recommended but not given (NG) 0.3%, treatment contraindicated (CI) 0.7%, no treatment (NT) 18.6% and unknown treatment status (UTS) 13.5%; for NH, CC 38.8%, SAC 10.5%, CNOS 14.5%, PRI 0.2%, REF 1.3%, NG 0.3%, CI 0.8%, NT 23.0% and UTS 10.4%. Regarding BMT/stem cell infusion, 3.1% H and 3.6 NH were confirmed to have received it; 2.5% H and 2.1% NH were confirmed to have received treatment involving radiation. Median survival was 3.7 years (y) and 3.8 y for H and NH respectively; the survival probability at 2 y was 0.65 (0.59-0.71) vs 0.65 (0.62-0.68), 5 y 0.40 (0.33-0.48) vs 0.41 (0.38-0.44) and 10 y 0.19 (0.12-0.30) vs 0.14 (0.09-0.21) for H and NH respectively. There was no statistically significant differences between the cohorts on stage of disease at diagnosis, types of treatment received or overall survival probability.
Conclusions: In Texas residents diagnosed with mantle cell lymphoma between 2006-2016, there were statistically significant differences in the level of poverty and insurance coverage between H and NH cohorts but no differences in stage at diagnosis, type of treatment received, or survival.
Diaz Duque:ADCT Therapeutics: Research Funding; Molecular Templates: Research Funding; AstraZeneca: Research Funding; Hutchinson Pharmaceuticals: Research Funding; Seattle Genetics: Speakers Bureau; Verastem: Speakers Bureau; AbbVie: Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal